Clinical Inquiry
A 3-year-old boy complained of vague abdominal pain, discomfort, and recurrent vomiting episodes, approximately every three months over the past two years.
The child was operated for malrotation in the early postnatal period.
Diagnosis :- Mid-gut volvulus

Discussion
Mid-gut volvulus, a complication of malrotation, occurs when the bowel twists clockwise around the superior mesenteric artery (SMA) axis due to a narrowed mesenteric attachment. Volvulus can lead to bowel obstruction, ischemia, or infarction, but its definition does not depend on the presence or absence of these complications.
Congenital malrotation of the midgut often presents within the first month of life. However, the overall incidence of malrotation is unknown, as some patients present years later or remain asymptomatic throughout their lives. Radiologists may encounter this diagnosis in various clinical settings, including incidental imaging findings, the cause of acute abdominal symptoms, or a condition associated with abdominal situs abnormalities.
Recurrent episodes of colicky abdominal pain with vomiting over months or years are typical and may eventually prompt imaging.
Bile-stained emesis and occasional bloody stools are key clinical indicators requiring rapid imaging investigation.
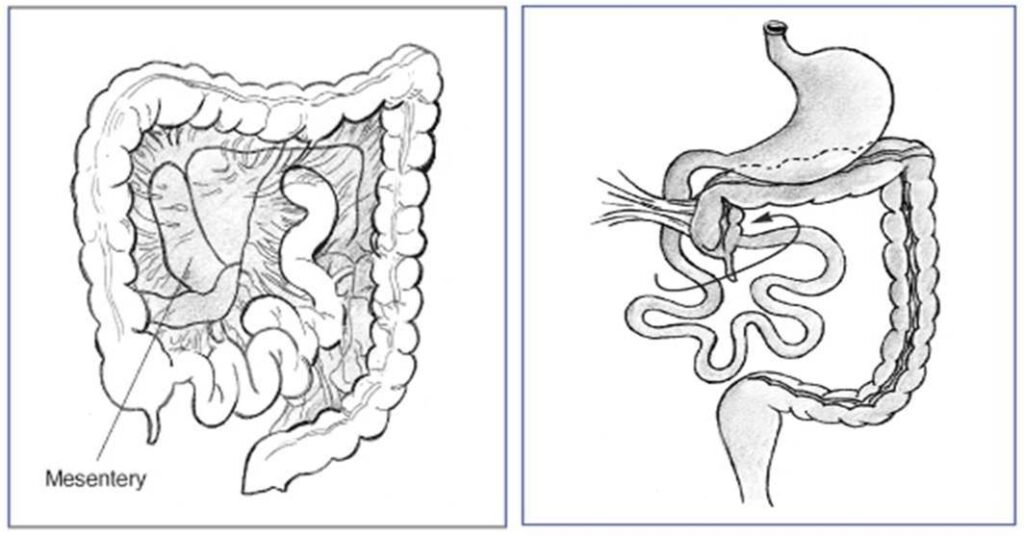
In the neonatal period, the normal mesentery has a broad base extending from the duodenojejunal junction (ligament of Treitz) in the left upper quadrant to the cecum in the right lower quadrant. Midgut malrotation encompasses a spectrum of congenital intestinal positional anomalies resulting from non-rotation or incomplete counterclockwise rotation of the primitive intestinal loop around the SMA axis during fetal development. This failure to complete rotation results in a narrow mesenteric base, predisposing the neonate to midgut volvulus (subsequent twisting of the bowel around the SMA).
The volvulus typically occurs in a clockwise direction. This is important to distinguish from other conditions, as Shimanuki et al. noted a counterclockwise whirlpool pattern in patients with enteritis.
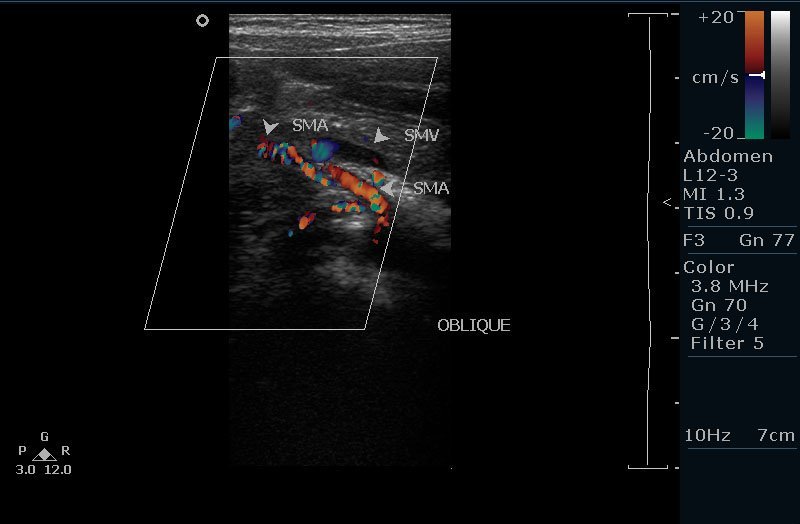
Ultrasound findings
Rule out hypertrophic pyloric stenosis. Then, the relationship between the SMA and SMV should be assessed. In the normal population, the SMV is typically located to the right of the SMA. The SMA is smaller, round, and surrounded by fat, while the SMV is larger and has a thinner wall. In malrotation/volvulus, the SMV is to the left of the SMA.
The whirlpool sign consists of a side-by-side arrangement of vessels with opposing flow directions, indicating that the whirlpool contains not only the SMV and its tributaries but also branches of the SMA.
Fetology
During fetal life, the duodenojejunal and ileocolic portions of the bowel normally rotate counterclockwise 270 degrees around the SMA. This results in the ileocolic valve being located in the right lower quadrant and the ligament of Treitz in the left upper quadrant.
In patients with malrotation, a narrowed mesenteric pedicle typically results in an abnormal position of the ligament of Treitz. This may be low lying, to the right of midline, and/or anteriorly located.
Associated anomalies are seen in approximately 60% of patients. These include congenital heart disease with heterotaxy (abnormal positioning and arrangement of abdominal organs, such as the spleen, liver, and major blood vessels) and right- or left-sided isomerism. Malrotation is almost always present in patients with congenital diaphragmatic hernia and abdominal wall defects, such as omphalocele and gastroschisis. It is also more common with other conditions, including imperforate anus, duodenal atresia, duodenal web, stenosis, pre-duodenal portal vein, annular pancreas, and biliary atresia.
The surgical procedure (Ladd procedure) involves reducing the volvulus and resecting any nonviable bowel. Ladd bands are transected, and the base of the mesentery is surgically broadened.
Fetal midgut volvulus
Fetal midgut volvulus has a specific clinical and echographic presentation. The primary maternal complaint is typically decreased or absent fetal movement. A non-stress test may reveal varying degrees of fetal distress. Ultrasound examination usually provides the diagnosis, demonstrating a characteristic whirlpool or snail-like configuration centrally located in the abdomen, often without peristalsis. Absence of blood flow within the central portion of the mass, as assessed by Doppler ultrasound, suggests gut ischemia. Intestinal necrosis and blood sequestration can be suspected by evaluating for fetal anemia, which may be initially indicated by abnormalities on the non-stress test and confirmed by Doppler velocimetry of the middle cerebral artery. Increased systolic velocity in the middle cerebral artery may suggest fetal anemia related to blood sequestration within the necrotic bowel loops. Polyhydramnios is a common sonographic finding in cases of obstruction. The timing of delivery depends on fetal lung maturity, the degree of fetal distress, and the ultrasound appearance of the fetal bowel. Delivery should occur in a tertiary care center, as immediate surgical correction of this anomaly is essential.
In summary, the whirlpool sign, visualized on transverse ultrasound studies, is a key indicator of midgut volvulus and allows for imaging-based diagnosis.
References
1. Pracros JP, Sann L, Genin G, et al. Ultrasound diagnosis of midgut volvulus: the “whirlpool” sign. Pediatr Radiol 1992;22:18-20.
2. Berdon WE. The diagnosis of malrotation and volvulus in the older child and adult: a trap for radiologists. Pediatr Radiol 1995;25:101-103.
3. Shimanuki Y, Aihara T, Takano H, et al. Clockwise whirlpool sign at color Doppler US: an objective and definite sign of midgut volvulus. Radiology 1996;199:261-264. reference
4. Buonomo C, Taylor GA, Share JC Kirks DT. Gastrointestinal Tract. In: Kirks DR, Griscom NT, eds. Practical pediatric imaging. Philadelphia, Pa: Lippincott-Raven, 1998; 857-865.
5. Bernstein SM, Russ PD. Midgut volvulus: a rare cause of acute abdomen in an adult patient. AJR Am J Roentgenol 1998;171:639-641.
6. Berdon WE. Midgut volvulus with whirlpool signs [letter]. AJR Am J Roentgenol 1999; 172:1689-1690.
7. Patino MO, Munden MM. Utility of the sonographic whirlpool sign in diagnosing midgut volvulus in patients with atypical clinical presentations. J Ultrasound Med 2004;23:397-401.
8. front malrotation without volvulus (studyblue.com)
9. medscape.com